The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Lege Artis Medicinae - 2023;33(8-9)
Content
Lege Artis Medicinae
SEPTEMBER 30, 2023




Lege Artis Medicinae
SEPTEMBER 30, 2023

Lege Artis Medicinae
SEPTEMBER 30, 2023

[The practice of periprocedural anticoagulation – birth of a local consensus]
[The problem of periprocedural anticoagulation is emerging more and more frequently in the day-to-day patient care. There is fundamental the interdisciplinary approach spanning the borders of different specialties by establishing the “anticoagulant team” including specialists as cardiologist, anesthesiologist and surgical experts for hands-on interventions (surgeon, traumatologist, obstetrician, endoscopic specialist etc.) and even the GPs as well. Such a communication can help considerably in the patient management and it would be useful to define local protocols and consensus papers adapted for the concerning hospitals. This review provides an overview of the points of considerations, the proposed practice of interruption and re-administration of oral anticuagulants, and the treatment of bleedings. ]
Lege Artis Medicinae
SEPTEMBER 30, 2023

[Hypertension and nephro-protection in elderly patients]
[The older people’s proportion and life expectancy is gradually increasing in our society, additionally the prevalence of hypertension and impaired kidney function can exceed 60 per cent in this age group. This study aims to highlight the importance of interrelation between hypertension and chronic kidney disease (CKD) and its adequate management, emphasizing professional considerations for the early recognizing and management of CKD, while keeping in mind the specific features of the ageing population in terms of prevention and therapy respectively. The overall mortality risk is higher in patients of advanced age, especially that of the elderly patient with CKD. This can increase their cardiovascular (CV) risk to such an extent that only a small proportion of patients with kidney disease reach the end-stage renal disease (ESRD) status. They die earlier by CV complications before having developed definite ESRD and needed renal replacement therapy. In conclusion, patients suffering from hypertension and CKD have a complex pathogenesis of cardiovascular risks and their CV risk is significantly higher, which requires increased caution and vigilance from the attending physician in the holistic care of elderly patients with kidney disease.]
Lege Artis Medicinae
SEPTEMBER 30, 2023

[Application of high-flow nasal oxygen therapy in the treatment of patients with respiratory failure caused by Covid-19 pneumonia outside the Intensive Care Unit]
[A significant number of studies addresses the benefits of high-flow nasal oxygen therapy (HFNO) in respiratory failure caused by Covid-19. However, the number among them about its use outside the intensive care unit is much less. Our study aims to evaluate the HFNO treatment data of patients with respiratory failure caused by Covid-19 in non-intensive care settings, and to compare them with three international studies and one local study with resembling subject.
To this retrospective cohort study, we selected patients with respiratory failure (n = 47) caused by Covid-19 pneumonia who were treated at the wards of the Sub-intensive Infectious Diseases Department, at Tolna County Balassa János Hospital, between March 16, and May 31, 2021. Exclusion criteria of starting HFNO therapy were low GCS (<13), multiple organ failure requiring intensive therapy, and hypercapnia (paCO2 > 50 mm Hg). With the patients’ general demographic data, we also evaluated treatment outcomes and mortality. We compared the duration of treatment and the average number of days of hospital stay with the number of care days among other patients not treated with HFNO, during the span of the study and the previous wave of the pandemic.
The patients’ mean age was 66 years (median: 67). The average duration of HFNO treatment was 6.829 days, which means a sum of 321 treatment days for 47 patients. 45% of the patients could be discharged home, 25% had to be transferred to the intensive care unit because they needed invasive ventilation, which was determined by a modified version of the national early warning score (NEWS) point system. Mortality during treatment was 30% and those of patients transferred to the intensive care unit mounted to 83%.
Compared with other three international studies and one local study, further based on our own experience, HFNO has proven to be effective in the treatment of patients with respiratory insufficiency not associated with hypercapnia caused by severe Covid-19. Based on patient feedback and nursing documentation, it increased the patient comfort compared with conventional oxygen therapy devices. Compared with data collected in the previous pandemic wave, the HFNO therapy reduced the average number of hospital treatment days and reduced the burden of the intensive care unit too.]
Lege Artis Medicinae
SEPTEMBER 30, 2023
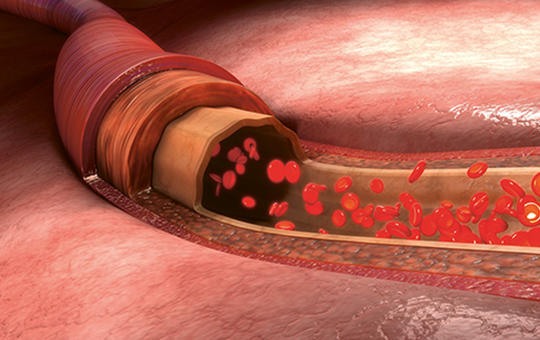
[Difficulties in recognising and treatment of lower extremity arterial disease in the elderly]
[
Cardiovascular disease is the most important cause of morbidity and mortality in elderly individuals worldwide. Lower extremity arterial disease is a diffuse degenerative process by atherosclerosis of the concerning arteries that can narrow or completely block the lumen of the arteries. One of the most important risk factors is the age, thus the occurrence of lower extremity arterial disease increases significantly with it exceeding 20% over the age of 70. The incidence of lower extremity arterial disease is mounting worldwide and one of the reasons for is the increase in the average age of the population. Recognition and also treatment of the disease show elderly characteristics, the knowledge of which is important in caring for increasing population of elderly patients with lower extremity arterial disease. Early detection and corresponding preventive treatment have a significant role also in this population. The wider range of intervention options can also provide an opportunity for elderly high-risk patients to avoid amputation and get a better quality of life.]
Lege Artis Medicinae
SEPTEMBER 30, 2023

[Could it be better?! – Methodological development of evaluation of the general practitioners’ performance ]
[Effectiveness in the primary care (PC) depends beyond the general practitioner’s (GP) personality and features of the practice on independent factors that are less weighted in our current performance evaluation scheme (PES).
Our goal was to demonstrate how the assessment of practice characteristics adjusted to the general practitioners’ performance would supplement the currently applied evaluation scheme.
We analysed the data from 2012 and 2018 based on the 12 indicators of the National Health Insurance Fund (NHIF). To assess the GPs’ professional performance, we developed indicators adjusted for sociodemographic status of patients and location of the practice and examined the dependence of the patients’ care on the GP’s performance.
According to the practice characteristics adjusted indicators, 43.5% and 21.8% of the GPs’ acknowledged by the NHIF had above-average performance. Those with average performance got bonus in 19.1% and 32.1%, meanwhile 15.3% and 27.9% of those with above-average performance were not appreciated by the NHIF score.
The current system is suitable for monitoring the patients’ care; however, the indicators reflect mainly the favourable conditions but underestimate the performance of disadvantaged practices.
The combined application of crude and adjusted indicators would be able to establish such a PES that could support a more effective interventions and a performance-stimulating financing system.]
Lege Artis Medicinae
SEPTEMBER 30, 2023
Lege Artis Medicinae
SEPTEMBER 30, 2023

Lege Artis Medicinae
SEPTEMBER 30, 2023

Lege Artis Medicinae
SEPTEMBER 30, 2023
1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
Clinical Oncology
[Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up]
29. AUG
3.
Clinical Oncology
[Pharmacovigilance landscape – Lessons from the past and opportunities for future]
29. AUG
4.
5.